Helpful Hepatic Hydrothorax Highlights: A Case Taken from the World of Twitter

Basic Management of Hepatic Hydrothorax
Referral for a liver transplant evaluation should be made while initiating treatment. Initial therapy should consist of sodium restriction (< 2 g/day) and diuretics. If the patient responds, great! If not, then we need to consider alternative invasive options including TIPS, repeated thoracentesis, pleurodesis or insertion of a chronic indwelling pleural catheter for drainage (see Figure 1).
Figure 1: Proposed Algorithm for Management of Hepatic Hydrothorax
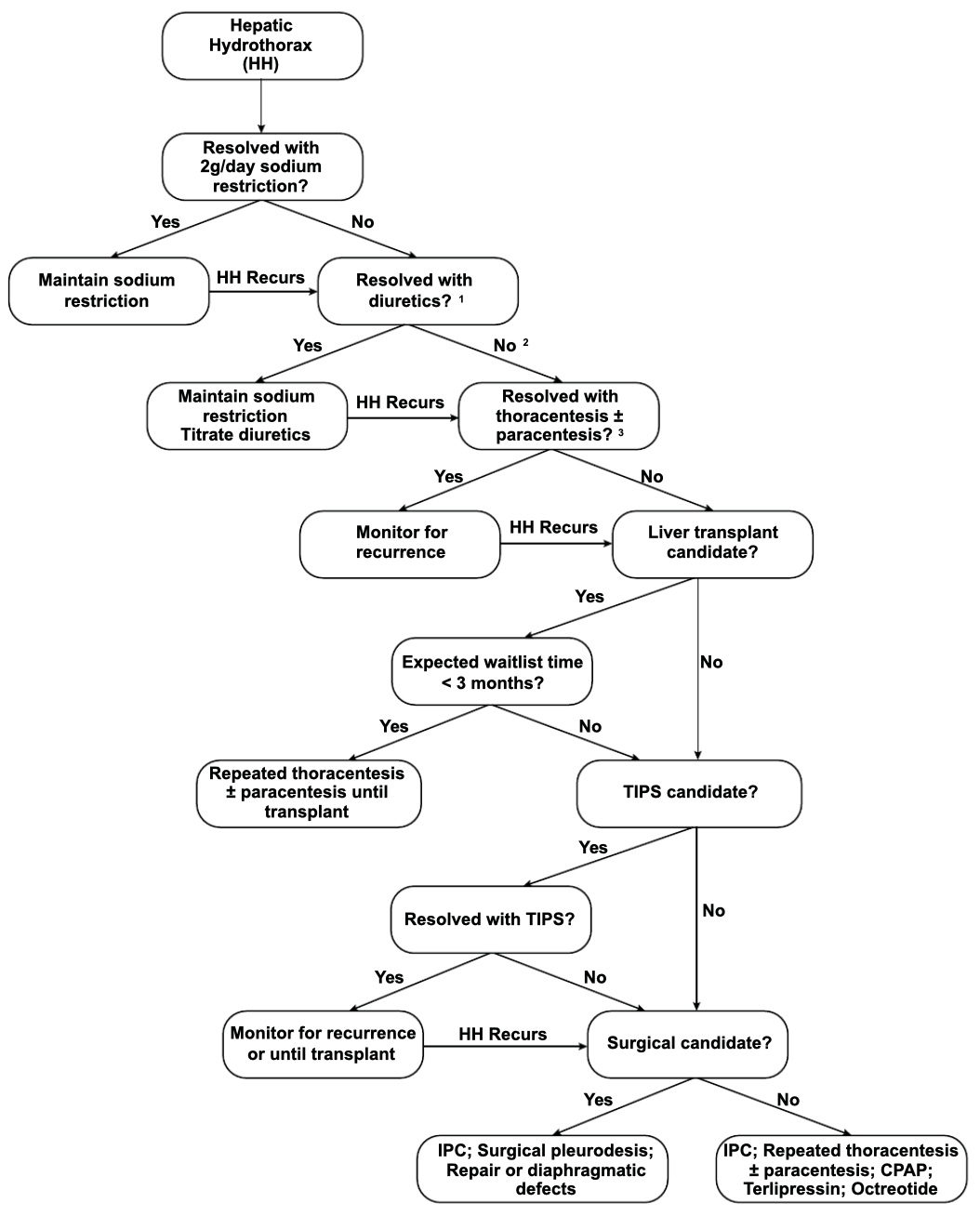
*IPC=indwelling pleural catheter
Taken from: Banini, B.A., et al., Multidisciplinary Management of Hepatic Hydrothorax in 2020: An Evidence-Based Review and Guidance. Hepatology, 2020
Options in REFRACTORY Hepatic Hydrothorax
20-30% of patients have persistent pleural effusions despite sodium restriction and diuretics. Treatment options include thoracentesis as needed, transjugular intrahepatic portosystemic shunt (TIPS), chronic pleural catheter drainage (i.e. PleurX), and/or liver transplant. Pleurodesis (ablation of space between parietal and visceral pleura) is rarely used and typically reserved when no other options exist.
Repeated thoracentesis:
- Can be helpful for fluid analysis and allow for rapid improvement of symptoms
- Complications and risks of thoracentesis include pneumothorax, hemothorax, air embolism, empyema, etc.
- Chances of these complications are higher in patients that will require repeated therapeutic thoracentesis.
Transjugular intrahepatic portosystemic shunt (TIPS):
- Can be lifesaving for some patients while awaiting liver transplant
- Success rates are between 42-79%
- Data is mainly from case series (see here, here, and here)
- Based on a systemic review, incidence of hepatic encephalopathy post TIPS for hydrothorax is 11.7% with a 17.7% 45-day mortality
- A study of 73 patients undergoing TIPS for hepatic hydrothorax found the following factors associated with higher mortality after TIPS placement:
- Pre-TIPS MELD >15
- Elevated pre-TIPS creatinine
- Lack of response in hydrothorax after TIPS placement
- Absolute and relative contraindications to TIPS are summarized in Table 1
Therefore, patient selection is key!
Table 1: Relative and absolute contraindications to TIPS

Taken from: Saab, Sammy MD, MPH; Kim, Nathan G. MD, MS; Lee, Edward Wolfgang MD, PhD. Practical Tips on TIPS. The American Journal of Gastroenterology: June 2020 - Volume 115 - Issue 6 - p 797-800
Transplant
- Transplant is the definitive treatment for hepatic hydrothorax and those without contraindications should be referred for evaluation
Indwelling pleural catheter
- Generally avoided due to complications of infection, pneumothorax, electrolyte and protein depletion, renal failure, etc
- However, on a case by case basis, can be used when patients decide that they want to focus their goals on comfort
Obliteration of pleural space and repair of diaphragmatic defects
- Pleurodesis involves ablation of space between parietal and visceral pleura
- Can be achieved by chemical means (i.e. use of a sclerosing agent) or mechanical means
- In a meta-analysis of 180 patients, a pooled complete response rate of 72% and complication rate of 82% occurred in those undergoing different methods of pleurodesis
- Surgical closure of diaphragmatic defect is an option but has significant limitations:
- Invasive; one study showed a 3-month mortality of 25%
- Diaphragm defects may be difficult to visualize
- Complications include septic shock, acute renal insufficiency, bowel ischemia and gastrointestinal bleeding
Table 2: Advantages and Disadvantages of Treatment Options in Refractory Hepatic Hydrothorax

Adapted from: Banini, B.A., et al., Multidisciplinary Management of Hepatic Hydrothorax in 2020: An Evidence-Based Review and Guidance. Hepatology, 2020