The Liver Biopsy: Importance and Interpretation

Why do patients get liver biopsies?
The main goals of a liver biopsy are to (1) render a diagnosis in a patient with abnormal liver function tests (LFTs) or a liver lesion on imaging, (2) provide staging and grading in a patient with a history of chronic hepatitis, (3) assess the liver’s response to treatment, and (4) assess the function of a liver transplant.
What type of liver biopsies do patients get?
Patients can have two types of liver biopsies: core needle biopsies or wedge biopsies.
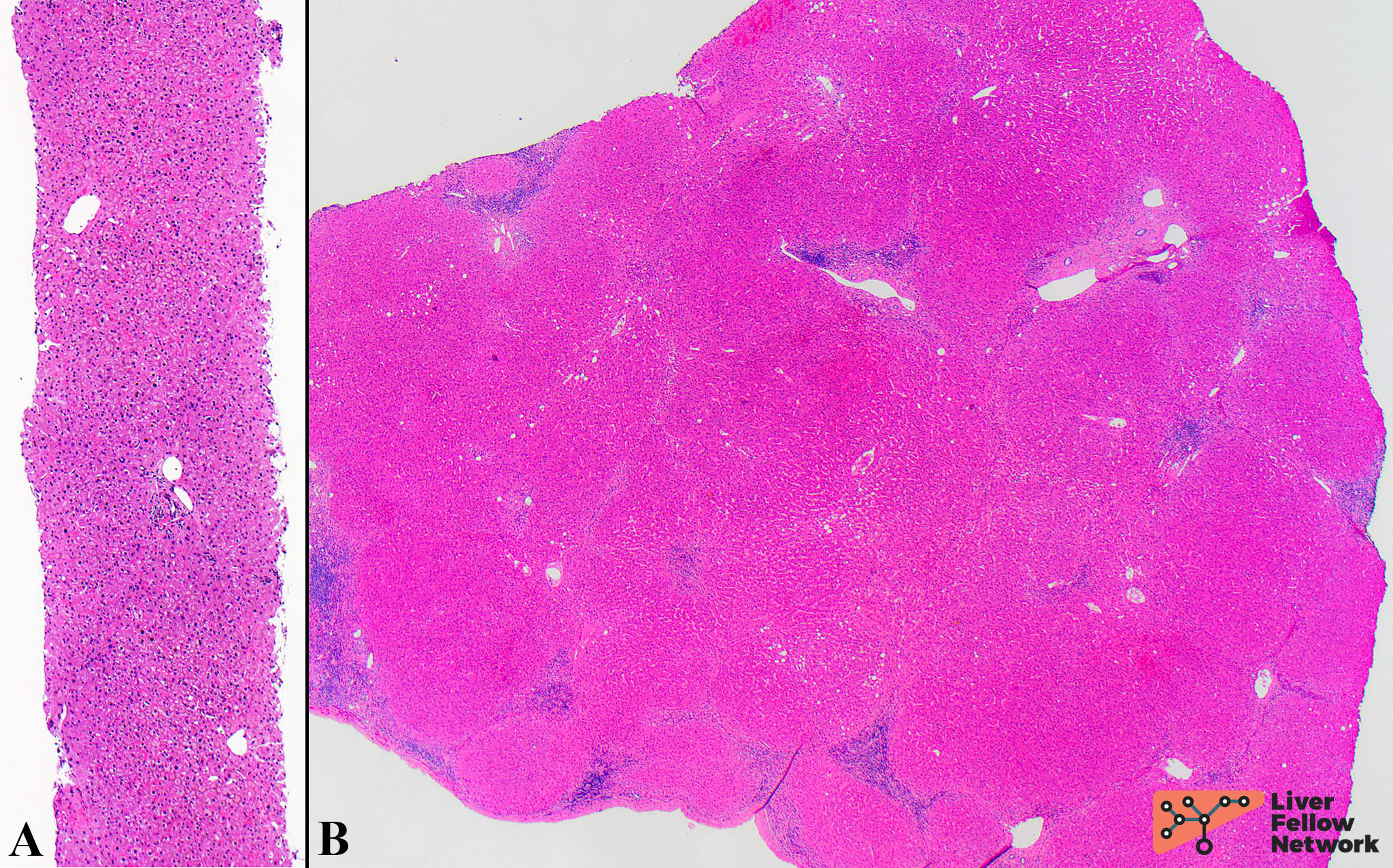
Core needle biopsies (Figure 1A) generate long cylindrical cores of liver parenchyma ~ 1 to 2 cm in length by ~ 0.2 cm in width. There are several approaches that may be used to obtain a core needle biopsy, including percutaneous, transjugular, laparoscopic or open, and image-guided. Percutaneous biopsy is the most common method. Transjugular biopsy is used in patients with a history of coagulopathy, significant ascites, or morbid obesity. Laparoscopic or open biopsies are taken when the patient is already undergoing surgery for another reason. Image-guided [via ultrasound or computed tomography (CT)] biopsy may be performed to target a specific lesion seen on imaging or when the other biopsy approaches have failed.
Wedge biopsies (Figure 1B) provide larger samples of tissue for pathologic interpretation. It is important to note that although there is more tissue available to assess, these biopsies are often subcapsular, which may give the false impression of increased fibrosis.
How do you interpret a liver biopsy?
Many pathologists first assess the liver biopsy without a clinical history so as to not bias the true interpretation. Once the biopsy has been assessed and a differential diagnosis formulated, then the microscopic findings can be correlated to the clinical history.
Step 1: Biopsy Adequacy
One of the first things to evaluate on a liver biopsy is whether the specimen is adequate. Although there are no formal “requirements” for evaluation of adequacy, it is usually assessed based upon the length of the core biopsy, biopsy fragmentation, and the number of portal tracts. Generally, most liver biopsies are 1-2 cm in length; however, studies have shown that biopsies at least 1.5 cm to 2.5 cm in length allow for better interpretation. Some liver biopsies may be fragmented when submitted for evaluation, either due to biopsy technique or due to the nature of the lesion (e.g., cirrhosis). In either case, the fragmentation may interfere with visualization of key histologic features. Lastly, many studies have tried to determine the minimum number of portal tracts needed to consider a liver biopsy adequate; however, the results are conflicting and range from 6 - 11 portal tracts. In all of the aforementioned cases, an inadequate biopsy may subject the patient to an additional procedure to obtain more tissue.
Step 2: Predominant Pattern
Pathologists interpret liver biopsies based upon histologic patterns, which have been well-described in the literature and are referenced at the end of this document. Here, we provide a brief step-wise approach for interpreting liver biopsies based on several patterns. Each pattern is associated with many etiologies. Further, patterns of injury can overlap. It is important to understand that this post is an overview and that these patterns are not all encompassing, but rather provide a basic framework for those new to liver pathology. Lastly, the entities associated with these patterns will be described in greater detail in future LFN Pathology Pearls posts.
LOBULAR PATTERN
The hallmark of the lobular pattern is “lobular disarray,” in which the normal architecture is disrupted due to injured hepatocytes (Figure 2A). This pattern is often characterized by lobular inflammation and hepatocyte necrosis. The inflammation is mainly mononuclear (lymphocytes and macrophages +/- eosinophils, neutrophils, or plasma cells) and can show focal lobular involvement or be more extensive. Additional findings include hepatocyte necrosis (spotty necrosis), dead/apoptotic hepatocytes (acidophilic bodies) (Figure 2B, 2C), and degenerating hepatocytes (ballooned hepatocytes) (Figure 2C). Cholestasis may also be present.
Common etiologies for the lobular pattern are viral hepatitis (hepatotropic viruses A-E, CMV, EBV, adenovirus, dengue, yellow fever), drug-induced hepatitis, and autoimmune hepatitis (AIH).

PORTAL PATTERN
The key histologic findings of the portal pattern include portal/periportal inflammation and fibrosis. The inflammation is mononuclear, but is predominantly lymphocytic (Figure 3A,3B). In some cases, lymphoid aggregates may also be seen. When the inflammation extends to the limiting plate (see post 1) and is associated with apoptotic hepatocytes, this is known as interface hepatitis. Some cases are associated with fibrosis that can progress to cirrhosis. The differential diagnosis for a portal pattern can be narrowed by identifying the presence/absence of additional histologic features (ex. increased plasma cells in AIH).
Common etiologies for the portal pattern include viral hepatitis (hepatitis C), AIH, drug/toxin-induced hepatitis, primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), and ⍺1-antitrypsin (A1AT) deficiency.

BILIARY PATTERN
The biliary pattern of injury displays a “ductular reaction,” which is characterized by the proliferation of bile ducts and inflammation within the portal tracts (Figure 4A, 4B). The ductular reaction may range from subtle to exuberant. The inflammatory infiltrate is mainly composed of neutrophils (Figure 4C). Additional findings may include fibrosis, edema, or cholestasis.
Common etiologies for the biliary pattern include large bile duct obstruction (strictures, atresia, stones), PSC, PBC, A1AT deficiency, and drug-induced injury.

STEATOTIC PATTERN
As its name implies, the steatotic pattern is characterized by steatosis, in which hepatocytes with intracytoplasmic fat are distributed throughout the lobules (Figure 5A, 5B). Macrovesicular steatosis is most common and is defined by larger fat droplets that push the nucleus to the periphery of the hepatocyte. In contrast, microvesicular steatosis is seen as a collection of smaller lipid droplets that surround a centrally-placed nucleus within the hepatocyte cytoplasm. When the steatosis is associated with ballooned hepatocytes and inflammation, this is known as steatohepatitis.
Common etiologies for the steatotic pattern include non-alcoholic steatohepatitis (NASH), alcoholic steatohepatitis (ASH), drug-induced hepatitis, and Wilson disease. Specifically, biopsies composed of mainly microvesicular steatosis are associated with Reye syndrome or acute fatty liver of pregnancy.

FIBROTIC PATTERN
The hallmark finding of the fibrotic pattern is dense eosinophilic fibrous bands that distort the liver parenchyma. Although it may be quite prominent on H&E, in some instances, it cannot be seen without the use of a trichrome stain. In most cases, fibrosis progresses from portal fibrosis to periportal fibrosis to bridging fibrosis and ultimately cirrhosis. There are several staging systems for fibrosis, but generally the lowest stage represents the least fibrosis (no/minimal fibrosis) and the highest stage represents the most fibrosis (cirrhosis). Cirrhosis is characterized by nodules of regenerating hepatocytes surrounded by fibrosis (Figure 6A, 6B). [Note: specific staging systems will be discussed in future posts].
Common etiologies associated with the fibrotic pattern include chronic viral hepatitis, drug-induced hepatitis, AIH, PSC, PBC, NASH, ASH, and Wilson disease.

NEOPLASTIC PATTERN
Neoplasms are often identified on imaging studies and can be benign or malignant. If malignant, the tumors can further be divided into primary or metastatic. Histologically, regardless of the type of tumor, the neoplastic pattern is characterized by a mass lesion that replaces the normal hepatic parenchyma (Figure 7A, 7B). When the microscopic findings suggest a metastatic lesion, a thorough investigation into the patient’s clinical history, as well as the application of immunohistochemistry, can be used to identify the site of origin.
Common benign neoplasms found in the liver include hepatic adenoma, regenerative or dysplastic nodule, focal nodular hyperplasia (FNH), and nodular regenerative hyperplasia (NRH). Malignant lesions include hepatocellular carcinoma (HCC), intrahepatic cholangiocarcinoma, metastasis (ex. colorectal carcinoma), and hepatoblastoma (children).

Step 3: Correlate
Identifying the main histologic pattern generates a list of potential diagnoses. Next, this list can be narrowed by comparing these microscopic findings with the patient’s medical history, radiologic studies, and laboratory findings. Some of the key laboratory findings to review include LFTs, viral serologies, and autoimmune studies.
Step 4: Special Stains & Immunostains
All pathology specimens are initially stained with hematoxylin and eosin (H&E). The hematoxylin imparts the blue/purple color (ex. nuclei), while the eosin imparts the pink color (ex. cytoplasm and extracellular matrix). Although a diagnosis can be rendered on H&E, in most cases the diagnosis is supported by additional special stains or immunostains. The most common special stains used on liver biopsies are trichrome, iron, reticulin, and PAS-D, while the most common immunostains are Hep Par 1, Arginase 1, glypican-3, cytokeratin (CK) 7, and CK19.
These stains will be discussed in more detail throughout future LFN Pathology Pearls posts.
Step 5: Render a Diagnosis
Liver biopsies for neoplastic lesions typically result in definitive diagnoses. In contrast, the diagnoses for medical liver biopsies frequently require the pathologist to provide a short list of differentials since, as detailed in this post, the microscopic features of many entities can overlap. The gastroenterologists/hepatologists can then correlate the pathologic findings with the patient’s clinical picture.
References
Chan, Y. Alwahab, C. Tilley, and N. Carr, “Percutaneous medical liver core biopsies: Correlation between tissue length and the number of portal tracts,” J. Clin. Pathol., 2010, doi: 10.1136/jcp.2010.076273.
D. Johnson, P. Laoveeravat, E. U. Yee, A. Perisetti, R. B. Thandassery, and B. Tharian, “Endoscopic ultrasound guided liver biopsy: Recent evidence,” World J. Gastrointest. Endosc., 2020, doi: 10.4253/wjge.v12.i3.83.
D. Odze and J. R. Goldblum, Surgical Pathology of the GI Tract, Liver, Biliary Tract, and Pancreas, Third Edit. Philadelphia: Saunders, 2015.
Saxena, Practical Hepatic Pathology: A Diagnostic Approach: Second Edition. 2017.
M. S. Torbenson, Atlas of Liver Pathology: A Pattern-Based Approach, First Edit. Philadelphia: Wolters Kluwer, 2020.