Normothermic Machine Perfusion

What are the benefits of using normothermic machine perfusion during liver transplant?
Normothermic machine perfusion (NMP) is associated with decreased risk of early allograft dysfunction, postreperfusion syndrome, ischemia reperfusion injury, and ischemic biliary complications compared to static cold storage. The ability to evaluate graft function during perfusion has also expanded the use of more marginal allografts and decreased organ discard rates.
How do these devices work?
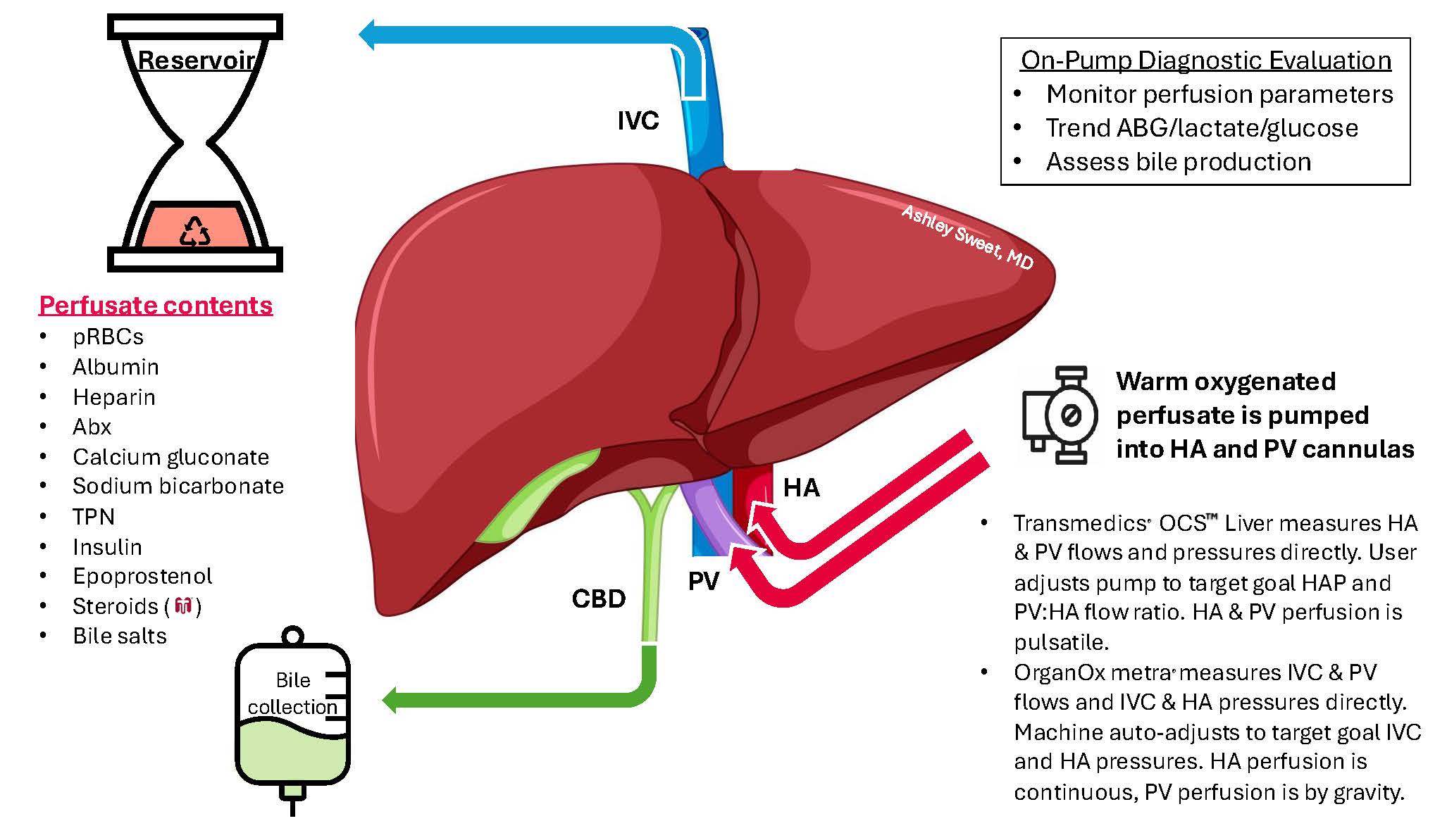
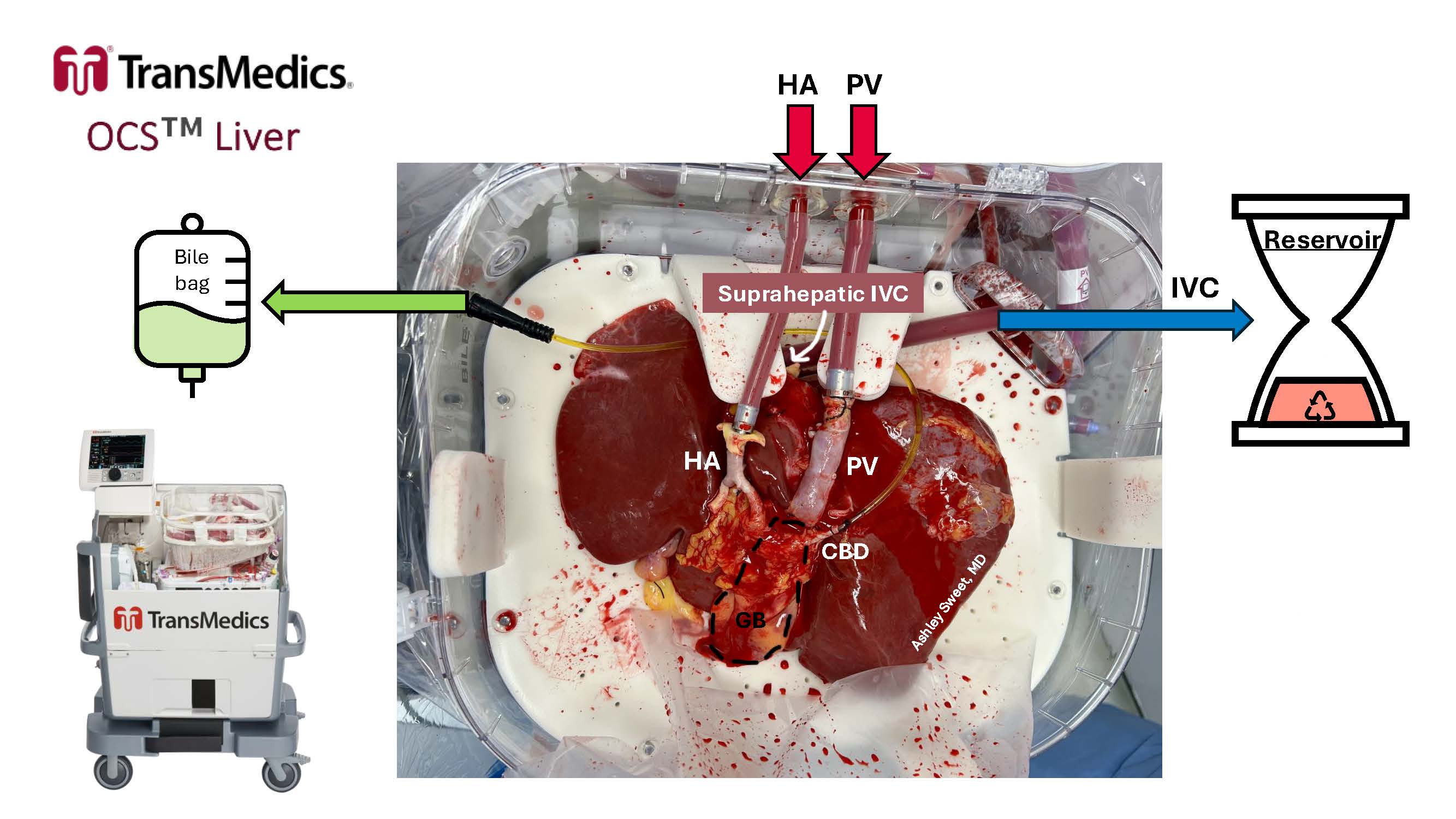
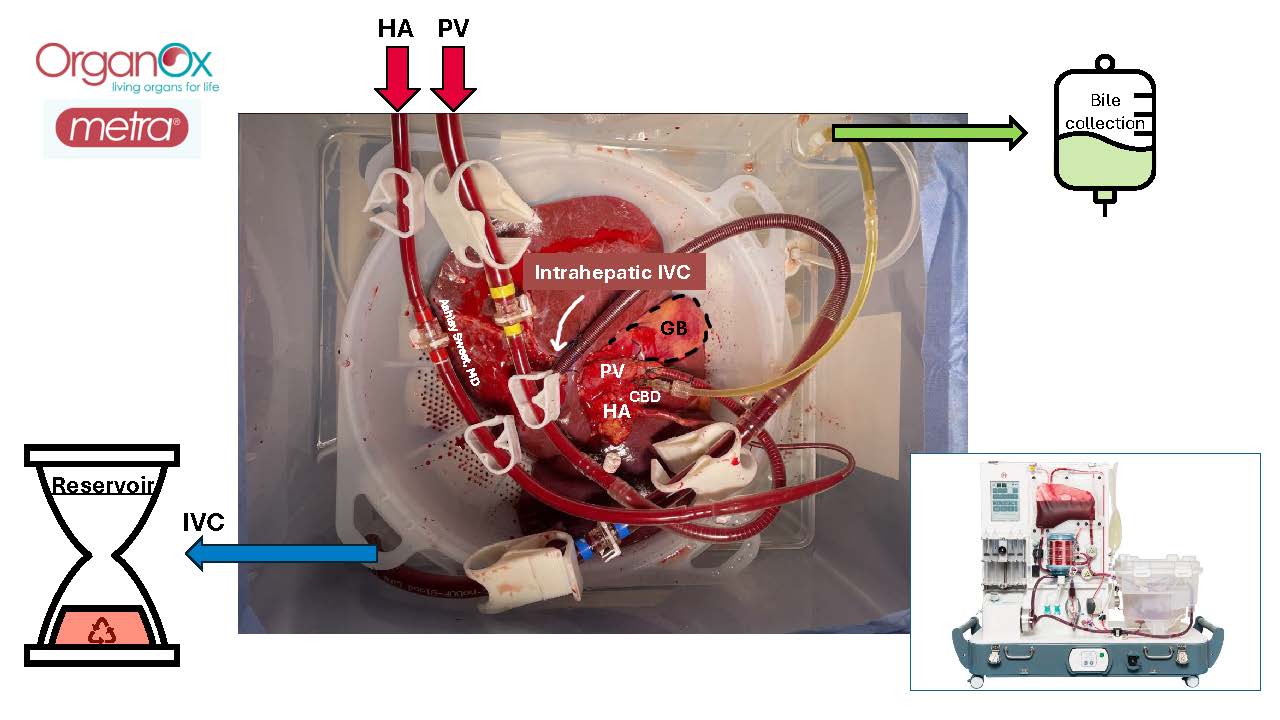
The graphics in Figures 1-3 depict how a liver is cannulated and connected to two commonly used NMP devices – the Transmedics® OCS Liver and the OrganOx metra®. In the Transmedics system, the suprahepatic inferior vena cava (IVC), portal vein (PV), hepatic artery (HA), and common bile duct (CBD) are cannulated prior to connection of the liver to the pump (Figure 2). In the OrganOx system, the infrahepatic IVC, PV, HA, and CBD are cannulated prior to connection, and the suprahepatic IVC is oversewn (Figure 3). Perfusion of the liver with warmed, oxygenated perfusate solution is begun and the perfusate recycles through the system.
Perfusate contents and perfusion parameters are summarized in Figure 1. In addition to the perfusion parameters, perfusate blood gas, lactate, and glucose are monitored during pumping. Adjustments can be made to meet the metabolic demands of the organ.